Multiple Sclerosis is an illness about which much remains unknown. Therefore, it is vital to be vigilant and detect the subtle and early signs of progression. In November 2025, Piet Eelen, Clinical Nurse Specialist at the National Multiple Sclerosis Center Melsbroek (Belgium), held a Webinar session in which he discussed these signs in detail. Among others, he talked about the current state of research, how to detect and assess progression, the role of nurses, and about improvements that could be made.
MS is a chronic, inflammatory and neurodegenerative autoimmune disorder of the central nervous system (CNS) affecting over 2.8 million people worldwide. It develops as a biological continuum: the pathological mechanisms driving disability are present early on. During relapse activity, PwMS may experience relapse-associated worsening (RAW), where symptoms deteriorate. With time, symptoms can improve, but even when DMTs are effective and reduce active inflammatory lesions on MRIs, disability may regardless progress. As the signs are less visible, it is a challenge to characterise PwMS whose disability is worsening.
Subtle disease progression is not adequately monitored by current clinical scales, such as the Expanded Disability Status Scale (EDSS). Changes in the general condition need to be recognised, recorded, reported so that it can be responded to accordingly.
This creates a need for a detailed step-by-step approach to identify disability progression regardless of age, EDSS or disease duration. Using this approach would help assess the presence or absence of certain variables to determine the stability or progression of the disease. Ultimately, this could contribute to more accurate treatment.
Relapsing-remitting MS (RRMS) is a type of multiple sclerosis where unpredictable relapses and remissions take turns. Disabilities resulting from relapsing can get resolved, but about 40% of attacks leads to permanent damage, odds of this growing with each passing year of the disease. Generally, 80% of PwMS have this variant.
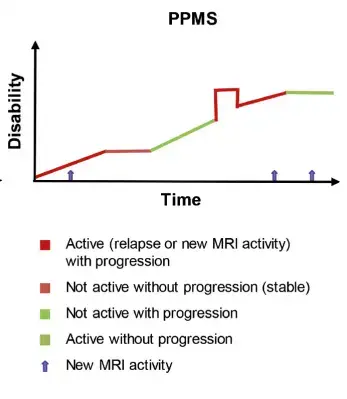
The difference between patients with RRMS and those with Primary-progressive MS is that the latter do not go through remission periods. Continuous worsening causes the progressive accumulation of disabilities. About 10-20% of PwMS suffer from this type.
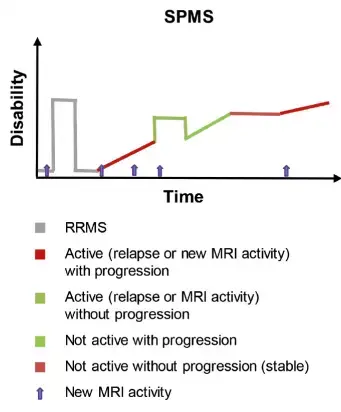
Secondary-progressive MS (SPMS) is a continuation of RRMS, where the definite periods of remission decline, giving way to continuous worsening. This progression appears in 65% of individuals with initial RRMS diagnosis.
Some important terms to take note of here are Relapse Associated Worsening (RAW) and Progression Independent of Relapse Activity (PIRA). The former describes the long-term accumulation of disability for PwMS as a result of neuroinflammatory smouldering and acute focal inflammatory events. The latter is defined as the "clinical manifestation of smouldering neuroinflammation.” It occurs behind an intact blood-brain barrier and is driven by intrinsic or trapped cells in the CNS, such as microglia or B cells.

Early detection is fundamental for the patient to receive the best possible medical care. The following section will explore the various aspects that can be used to confirm a diagnosis of progression, including clinical assessments, input from cognitive, Patient Recorded Outcomes (PROs), and imaging assessments.
One of the easiest but most fundamental assessments is functional testing, for instance Patient Recorded Outcomes (PROs). They track objective as well as subjective measures through active data gathering practices like questionnaires, or passive data gathering practices like registrations. Different PROs evaluate different aspects of MS symptoms, including walking, cognition, pain, bowel and bladder, or quality of life, so healthcare professionals can choose what type to use. The result of multiple patients can also be aggregated into group results which could provide a clearer, generalised understanding of these symptoms. In spite these positives, it is still uncertain to what extent PROs can contribute to clinical change.
The initial evaluation must take into account additional factors like age, sex, smoking status, and the presence of comorbidities (eg. cardiovascular disease, obesity, psychiatric disorders) and exclude external factors potentially affecting the functioning of the patient (eg. menopause, ongoing infection, stress, depression).
Accurate tracking is crucial to identify changes since last visit and nurses must ask specific questions to get a full picture of all alterations that the patient might not even recognise or disclose. If, based on the tests, it is concluded that the patient in question is at risk of disability progression, further steps must urgently be taken.
Domains to check to uncover disability progression:
Physical tests |
|
| Patient-reported outcomes |
|
| Optical coherence tomography |
|
| Walking ability |
|
| Magnetic resonance imaging |
|
| Cognitive tests |
|
| Clinical biomarkers |
|
The most important component in detecting progression is conversation. It is necessary that nurses think proactively about their patients and that they are part of MDTs to facilitate individual roles. Though, nurses might still find it difficult to "translate” the scientific reality in a clear and understandable way for the patient. MS Nurse Pro provides education and training aimed at this. As a free resource, it alleviates some of the resource constraints restricting nurses.
Other constraints include too little time, too much administrative work, shift work, working in different departments, and working with interim nurses. These limit nurses’ capacity to organise more frequent and in-depth consultations, and formal assessments, attend trainings or closely collaborate with neurologists. Staff shortages also mean each nurse will have to care for more patients. Further hindering care is the often-insufficient level of knowledge of novice, interim, or even registered nurses. With less knowledge and experience, they are less likely to be able to notice and detect early signs of progression. In addition to this are systemic barriers, such as limited access to specialists, fragmented care coordination, insurance or reimbursement issues, inadequate health record integration and limited multi-disciplinary support.

First, the role of advanced nurses (eg. clinical nurse specialists and nurse practitioners) must be expanded, combined with establishing a stable MDT that follows the patient throughout their journey.
Second, increasing knowledge would be a cornerstone improvement. This strategy could comprise of enhancing the knowledge and competences of nurses themselves, but that of patients as well. Similarly, regular visits, ongoing conversation with PwMS, and better documentation could be considered as part of this second step.
Third, the wars of working must be reformed through: